This isn’t something that the people in Dell Rapids read every day in their public notices:
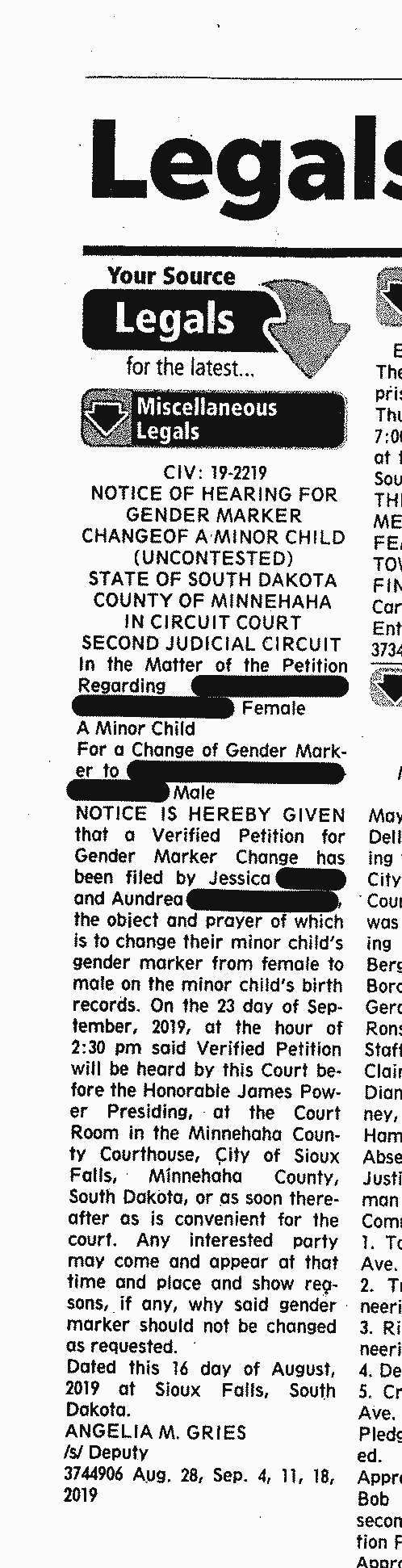
A hearing has been noticed for September 23rd at the Minnehaha County Courthouse that the parents of a 13 year old girl are petitioning the court to change the child’s “gender marker” from “female to male on the minor child’s birth records.”
The court filings in this matter are even more interesting. (I have redacted information, as it involves a minor child):
Gender Change Petition Etc – Judge Power Case by Pat Powers on Scribd
While the name change portion of the petition was granted by Judge James Power, the portion of the decision referring to “gender marker” was scratched out on the paperwork, and it appears to have been noticed for hearing.
Why? There’s no such thing as “gender marker” in South Dakota state law.
The term “gender marker” itself seems to have arisen only in the last couple of years in reference to discussions about changing the designation of sex on official documents. “Sex” in the gender reference is a biological reference, where “gender marker” seems to be more of what people trying to change it are calling a reference to a legal status.
If South Dakota is going to open the door to “gender status” it opens up an entire can of worms that the state has not touched on yet in terms of changing legal designations of gender.
And that’s just the start of it. Because this legal filing may also shock the legislature to action.
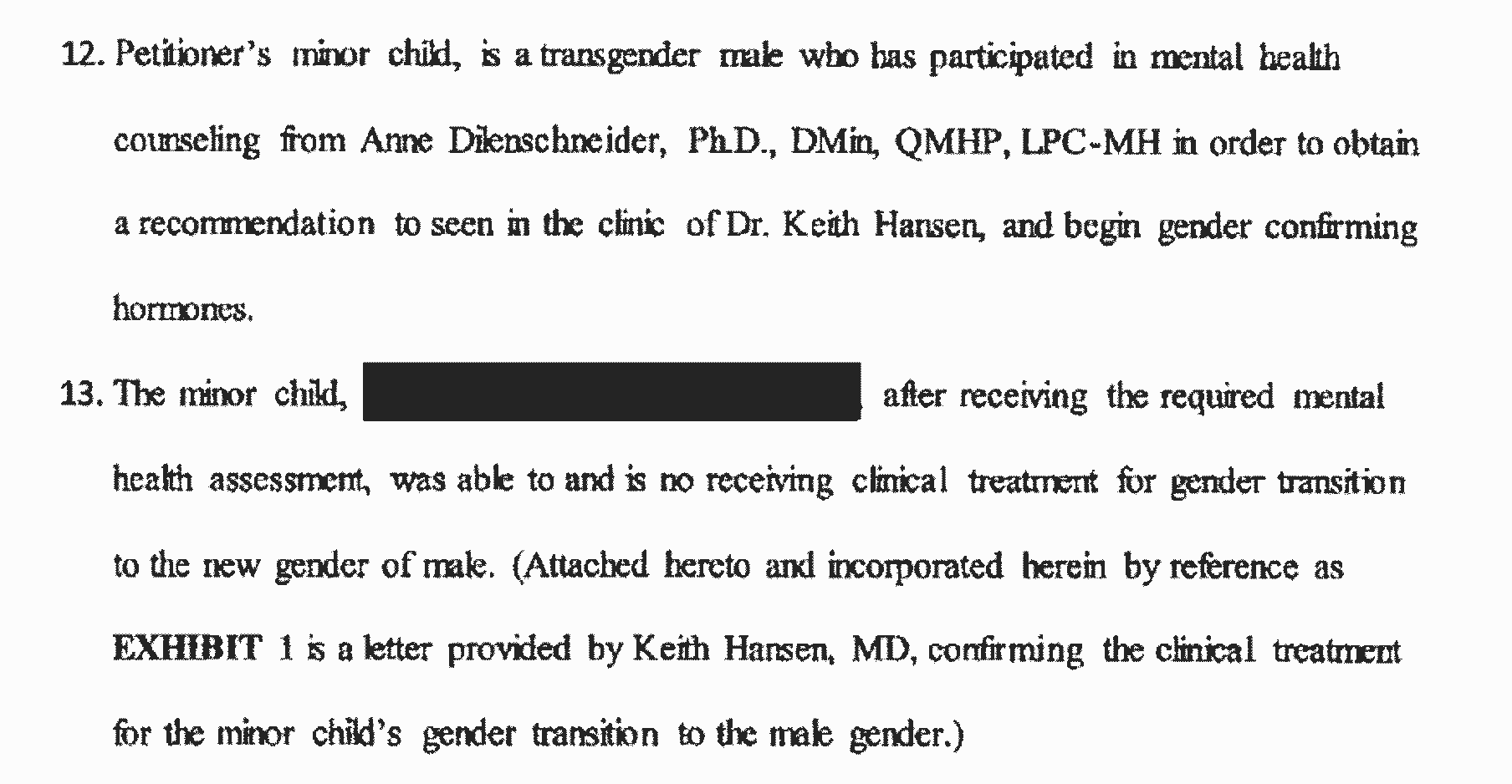
Contained as part of the court documents, it describes that this 13 year old minor child has prepared for and appears to be receiving hormones for gender reassignment:
This court filing may be the first hard evidence as to the fact that gender reassignment treatments are actively being performed in South Dakota on minor children. And that’s important because this topic is one we’re going to hear about it this next legislative session.
Under a comment on this website back on July 25th, State Representative Fred Deutsch made note of his intention to bring legislation this next session that would regulate the procedures the parents in this matter intend to allow to be conducted on their child:
Next session I will bring a bill with the similar purpose of protecting South Dakota children from dangerous, unscientific and life-altering medical procedures pertaining to sex and so-called gender identity. I’ll take a different approach, and hope I can prove to the legislature, the governor, and the people that the bill is important and necessary.
South Dakota may find that this could be one of the major fights of the upcoming legislative session.
Going beyond the choices an able bodied adult makes for themselves, the fact that these medical procedures are something that parents are asking/allowing to be performed on minor children as young as 13 years old is shocking to the conscience of many.
Stay tuned for more on this as the story develops.
No basis in the law for the change…should be a short hearing.
I stand with President Trump………..https://www.youtube.com/watch?v=3dXBeUxvkW8
https://www.washingtonpost.com/news/post-nation/wp/2017/03/30/north-carolina-lawmakers-say-theyve-agreed-on-a-deal-to-repeal-the-bathroom-bill/?noredirect=on
Testosterone is being given in extraordinarily high doses to females with confusion about their sex. Testosterone is being administered to bring levels on the order of 10-40X higher than the normal adult female range. The health consequences include increased risk of heart attack and death due to cardiovascular disease, erythrocytosis (high red blood cell counts), severe liver dysfunction, hypertension, infertility, and increased risk of breast, uterine, and ovarian cancer.
High dose testosterone also has a multitude of pyschological effects. Studies have shown:
– 23% of subjects using high doses of anabolic steroids [such as testosterone] met DSM criteria for a major mood syndrome (mania, hypomania, and major depression)
– 3.4-12% developed psychotic symptoms
It is known that psychiatric symptoms become more common and severe as the dose increases.
This is an extraordinarily dangerous treatment for females. There is no FDA approval for this use and there have been no long term studies done to determine efficacy or safety. This is a form of physical conversion therapy that will cause lasting physical and mental harm to adolescent and adult females.
Read more here:
http://gdworkinggroup.org/2018/10/24/the-gender-identity-phantom/
Thank you, Dr. Laidlaw.
So Dr. Laidlaw, what makes you so interested in SD. Don’t you practice in CA?
I am not opposed to trans rights; but I do believe those rights must be balanced against children’s right to be protected from harm. Children suffering from gender dysphoria should have access to the full compliment of a mental healthcare provider’s training; but those providers that refer for mutilating sex procedures, and the so-called doctors that perform them, should serve time behind bars and pemantly lose the privelidge to practice medicine in SD.
We don’t let kids in high school smoke, drink, play video lottery, buy scratch cards, gamble in deadwood, get married, enter into a contract, or under the age of 16 engage in sexual contact, but somehow we think they are wise enough to take hormones that permanently alters their bodies and makes them sterile. How can a child possibly understand the risks? How can a child possibly provide “informed consent.” This medical practice is horrendous and should be illegal. Shame on the doctors that do this. Shame on Sandford and RC Region for employing these doctors.
“Next session I will bring a bill with the similar purpose of protecting South Dakota children from dangerous, unscientific and life-altering medical procedures pertaining to sex and so-called gender identity. I’ll take a different approach, and hope I can prove to the legislature, the governor, and the people that the bill is important and necessary.” quote FD……..Fred why don’t you just come out and be up front. This bill is to protect children from their parents.
I must say this is what bothers me a lot. That people are undergoing medical procedures without all the information needed to make consent, or just too young to make a valid decision. People suffering are turned into life-long commodities by Frankensteinian doctors.
IMO, this is likely more about the parents’ issues that they are projecting on their child.
For starters I’d suggest that this muddling of sex & gender & nonsense like “gender assigned at birth” will promote & induce confusion & dysphoria in vulnerable children, all to the vast profit of the pharmaceutical & medical industries
Tara this is child abuse. Open your eyes. If you don’t agree, what would it take to become so? A mastectomy? I hope Sanford and RCR aren’t doing those too
I agree, but it is to bad the government is making decisions when the parents should be protecting their children from sex changes. When the kid turns 18, then they can do what they want.
Ignorance right here. This doctor would rather pump SD kids with hormones & schedule their barbaric surgical procedures rather than tell a child they are beautiful the way they are
Don’t blame the Dr. It’s the parents. I hope they don’t waste their time in Pierre over sex bills. The government should stay out of people’s sex identity issues.
For crying out loud, the kid is 13! And you want the state to just stay out of it? No wonder you can’t win an election – you have no common sense.
Like Government is going to solve our problems. My common sense tells me government is a joke.
Is that why Ron kept running for office?
Perfect example how screwed up children have become since the Supreme Court legalized gay marriage. Anyone else notice the two parents, now divorced, are both women? The child’s biologic father gave up his parental rights. Now this 13 year old child doesn’t know if she is a boy or a girl. Poor kid. She never had a chance for a normal life. Father isn’t in the picture and the two “moms” are now divorced. Liberals want the world to believe traditional marriage between a man and a woman isn’t important. But this is the type of stuff that happens when you start screwing with the family. Who pays the price? Children.
There it is, the typical right-wing screed with little to no relation to the topic at hand…
Traditional marriages can screw up kids too.
Cats & Dogs living together. Total chaos! What is this world coming too?
Maybe you shouldn’t have a family given your backwoods, prairie primitive views on something that doesn’t affect you at all.
Also, I don’t disagree with many of Pat’s postings – but don’t think this one rises to the standard of needing a post. I also think Mr. Deutsch often seeks to legislate when there isn’t a problem- but then again i’d never vote for him as a Republican because I think his views on most things are too dated.
When did what someone else does in their private lives affect you and you marriage so much that you need to openly attack others? I also appreciate how you draw so many inferences about what the child is like or is going through without knowing the individual first hand.
Who pays the price when parents cant afford food or basic necessities? Who pays the price when children are brought into the world to parents who are suffer from substance or mental health diagnosis? Who pays the price when children don’t get a decent education?
Having same-sex parents is no different that having two parents of different sexes, all families have issues. What mattes more- having loving parents or just having a mom and a dad?
You must be from one of those advanced progressive states that celebrate abortion and the like. For me, I’m thankful South Dakota has legislators with the guts to bring bills on important social issues that protect and conserve our values.
“Also, I don’t disagree with many of Pat’s postings – but don’t think this one rises to the standard of needing a post.”
Obviously, I would disagree, as it is newsworthy for a few reasons.
First, it’s breaking new ground in petitioning the state for changing a “gender marker,” and already that’s a problem, because “gender marker” is not described in law. Gender Marker is more of a legal designation, versus what’s in SD law, which is “Sex” referring to biology. If we think this issue is going away, it isn’t. It’s something that’s been seen in other states, and it may become more common.
Second, the topic of sex reassignment for minors and it’s legality is going to be a hot button issue this next legislative session. It started to come up last session, but probably wasn’t ripe. Now, the legislature has a case of it taking place.
Agree or disagree, these issues are going to be argued and debated for some time to come.
Agree. This is 100% newsworthy. This is a huge problem that needs to be addressed. Liberals want us to look the other way, but our kids deserve better than to be experimented on by activist parents and doctors.
Tara, this is the deliberate sterilization of a 13 year old girl. It isn’t just some “identity” thing like picking one of 72 genders on Facebook. “Identify” in whatever detached-from-reality way you want. But don’t (1) try to alter a factual record to reflect your unreality; and (2) sterilizing middle schoolers is not ok.
That’s disgusting and I agree, a child should never be put through that.
Aren’t there already laws on books protecting children?
Am I reading correctly that two lesbians want to have a sex change for the child? The article states that one is the biological mom and one is the adoptive. Both have women’s names. No child age 13 is capable of giving this kind of consent and the judge should be questioning the child about being mentally abused into believing that such a life change would lead to any kind of normalcy at all. I think this procedure would have a doomed outcome and the mental chaos would still remain.
These are kids. Kids. My God, what kind of doctors do we allow into South Dakota?
The laws are already in place and the Judge probably will not rule in favor of the parents. Less laws, not more. Focus on sex-trafficking, sexual abuse, abduction of children from their families, DSS, and smaller government. Too spend weeks on an isolated issue about a sex change is throwing red meat out to your base. Oh that’s right, it’s campaign season rolling around again.
We urge South Dakotans to examine what is happening throughout the country and take action before it is too late. There is an epidemic of teens now identifying as transgender. A recent CDC survey showed nearly 2% identify as transgender, while an additional 1.6% believe they might be. What was once a rare phenomenon is rapidly spreading.
Most concerning is the fact that harmful hormonal and irreversible surgical interventions are being performed on gender-nonconforming children without one single long-term study to support their safety or efficacy. Clinicians are now administering powerful puberty-blocking drugs and cross-sex hormones to a growing number of gender non-conforming pre-adolescents. “Gender-confirming” surgeries — including mastectomies, radical hysterectomies, vaginoplasties, and orchiectomies — are now being performed on teenagers.
Parents who consent to these treatments are often misled to believe that their child will be at greater risk of suicide if they do not. There is no evidence to support this claim.
Young adults are also at risk of hasty medicalization. An increasing number of “informed consent” clinics provide cross-sex hormones to young people after only one or two visits. These clinics do not require mental or physical health assessments. Surgeries may be obtained within months.
In the past, hormones and surgeries were offered only to adults with a lifelong history of severe and unremitting distress, and only after extensive medical and psychological screening. Yet these same life-altering medical procedures are now offered to young people based on feelings that are likely to change with time, brain maturity, and non-invasive therapy.
The medical literature on the health effects of hormonal interventions “in the pediatric/adolescent population is completely lacking.” A recent large cohort study, which tracked nearly 4,000 transgender-identifying adults receiving hormone therapy for an average of eight years, found that women’s risk of heart attack tripled while men’s risk of developing venous thromboembolism became five times greater. The full extent of the medical harms of hormonal treatments — prescribed for lifetime usage — will not be realized for many years.
The only long-term follow-up study among adults who surgically transitioned found substantially higher rates of overall mortality, suicide, suicide attempts, and psychiatric hospitalizations. These risks did not become apparent until ten years after transition.
An increasing number of young people are beginning to express their painful regret of surgeries and hormonal interventions that have irreversibly impacted their health, appearance, fertility, and sexual function. Many report that they did not receive proper counseling and were not encouraged to consider non-invasive options.
Young people should not be offered life-altering hormonal and surgical interventions that are not supported by rigorous studies establishing long-term efficacy and safety. The risks of irreparable harm and regret are too great.
We hope that courageous lawmakers will put an end to this medical scandal. Please see our website for more information: http://www.KelseyCoalition.org
Media Matters appears to challenge The Kelsey Coalition and Dr. Laidlaw in spreading misinformation with classic fear mongering. https://www.mediamatters.org/heritage-foundation/anti-trans-parent-group-kelsey-coalition-usa-today
Would this be the Media Matters as funded by Moveon.org and George Soros?
https://en.wikipedia.org/wiki/Media_Matters_for_America
How many children in SD have already had sex changes?
American Academy of Pediatrics
Transgender Adolescent Suicide Behavior
Russell B. Toomey, Amy K. Syvertsen, Maura Shramko
RESULTS: Nearly 14% of adolescents reported a previous suicide attempt; disparities by gender identity in suicide attempts were found. Female to male adolescents reported the highest rate of attempted suicide (50.8%), followed by adolescents who identified as not exclusively male or female (41.8%), male to female adolescents (29.9%), questioning adolescents (27.9%), female adolescents (17.6%), and male adolescents (9.8%).
9:34 am Understand your data. What you cite is raw data and in the authors’ own terms does not examine underlying causes. As a basic principle of rational inquiry, you cannot surmise any causation from correlative data. The study’s prime author, Dr. Toomey, explains that he doesn’t understand the causes of these suicide statistics: he says there’s a, QUOTE, “urgent need to understand why transgender, female to male, and nonbinary adolescents report engaging in suicide behavior at higher levels than other adolescent transgender populations.” Sure, let’s study it. But let’s not engage in wholesale medical experimentation on 13 year old girls.
Perhaps it’s caused by co-morbidities with other psychological disorders, or perhaps because the gender identity disorder is itself ipso facto distressing? Perhaps not. But the leading long-term study on the topic shows huge disparity in suicide (>19x for completely “transitioned”), even in the very “affirming” environment of the study location (Sweden). https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0016885
This WSJ op-ed may require subscriber status. If so, I apologize. The short summary is that Johns Hopkins was both an early adopter of gender reassignment surgery and among the first to abandon it for medical reasons. In short, it didn’t achieve the psychological ends anticipated and there was no physical justification for it. See: https://www.wsj.com/articles/paul-mchugh-transgender-surgery-isnt-the-solution-1402615120
So let the parents, coaches, psychologists deal with it locally. Go back to local control and keep these part-time politicians out of it. Focus on property tax relief, lowering college tuition, health care and thing that affect the state as a whole. Thanks. Genital issues should be a private matter.
Tara, you’re nuts. Local control f what? This has noting to dowith local control. It’s all about the safety of children. You’re out of your league, lady. You don’t know what you’re talking about.
Go a head and put your faith in Government. If you think I am nuts for letting government decide on personal issues, well so be it. I would rather debate than hate against people who don’t agree. People that resort to name calling and who hid behind a fake name is pretty classless.
Says the woman that keeps running for government but doesn’t have the trust of the people to win an election.
That’s their own damn fault when over 80% don’t show up to vote…..then don’t complain.
Thanks for sharing Michael. The researcher in me finds this an interesting topic that’s atypical from the usual political discussion we have in SD, so I’ve been googling and seaching pubmed for orignal research, comprehensive reviews and metastudies to learn more. In agreement with your wsj link, I have not been able to find any long-term scientific evidence that struggling children and youth benefit psychologically from these body-transforming procedures. One of the more recent comprehensive literature reviews was published earlier this year by the Editor in Chief of the British Medical Journal and Professor of Evidence Based Medicine. He described puberty blockers for gender dysphoria being used “in the context of profound scientific ignorance,” and as a “momentous step in the dark.” The review concluded “the current evidence base does not support informed decision making and safe practice in children.” Again, fascinating discussion. I look forward to seeing what the legislature does to protect our children from these poorly supported life-transforming medical procedures.
Lots of jumping to conclusions here – shocker!
I don’t see anywhere in any of the documentation that testosterone or irreversible treatments are to be given. The court filing merely mentions “hormones” – most likely Leuprorelin – a ‘puberty blocker’. From what I’ve read on the matter, outside of a loss of bone density and some very mild side effects, the treatment would be reversible if this young person decides to forego the transition down the line. Testosterone/estrogen/etc. are not indicated for children under 16, so that bridge will be crossed at a later date. I did not see any mention of surgery (if I’m wrong on that, please point out the relevant section).
As to the parental genders – who cares? You simply can’t draw any conclusions about how or if the parents have influenced the child’s decision in any way whatsoever. Once you’re down that particular road, you’re lost. Children need loving homes, and that’s pretty much the end of it.
If a minor wants to transition to the opposite gender and their parents are not supportive of this process is the child in a “loving” home?
You open the door for a teacher/counselor to claim a minor must be removed from their home, taken from their parents, because their definition of “loving home” is different from the parents. Ohio parents lost custody of their child because they refused to give her transgender drugs. This is not pretty much the end of it.
Walt Heyer could give you some perspective about how abusive people who support and encourage this process are, and you clearly need some perspective.
This is the stupidest thing I’ve heard today. So if my kid wants a pony, CPS will remove the child from my home since I don’t love them? What about parents who refuse to vaccinate their kids?
…and I’m aware of Walt Heyer. He’s making bank off his previous mental illness, but – dissociative disorder =/= gender dysphoria. He blames one of his “feminine personalities” (even refers to her in the 3rd person) for going through with the surgeries (dude, that girl is YOU). This is akin to saying that since my mom passed away, all people suffering from depression have lost a loved one. He’s also a religious nutter, so that gives him another big axe to grind, and another reason to doubt his veracity.
Walt Heyer’s life is a tragedy not doubt and found out he made a mistake but Walt is an extremely small minority. Now this is Walt’s gig and he is burning down everyone around him for money and some fringe fame.
Walt Heyer is making everyone else pay for his mistake. Desperation can bring out the worst of people.
Right up there with college students. Are culture has changed from a couple of generations ago……https://www.cbsnews.com/news/1-in-5-college-students-so-stressed-they-consider-suicide/
our
I’ll take the word of the doctor that commented above.
There are many more doctors who disagree. Are their words worth less simply because of your confirmation bias? Perhaps you should seek a second opinion.
Ike, first, look at the petition paragraph 12: “in order to … begin gender confirming hormones.” “Gender confirming hormones,” not puberty-suppressing. That would mean testosterone for this 13 year old girl, wouldn’t it? That’s certainly the plain reading of it.
Second, platitudes aside, the data isn’t in dispute — it’s not just about “loving homes”; outcomes for kids are vastly better across a range of metrics when they’re raised by a mom and a dad. http://www.baylorisr.org/wp-content/uploads/Regnerus.pdf Dr. Regnerus: “The [study] results reveal numerous, consistent differences, [e.g. in education, behavior, and emotional well-being] especially between the children of women who have had a lesbian relationship and those with still-married (heterosexual) biological parents.”
Gender-confirming hormones like leuprorelin would absolutely fall under that description:
“The World Professional Association for Transgender Health’s standards of care recommend suspending puberty, preferably with the use of gonadotropin-releasing hormone agonists, in certain gender non-conforming minors (aged under 18 years) who have undergone a psychiatric assessment and have reached at least Tanner stage II of puberty. This approach seeks to lessen the discordance between assigned natal sex and gender identity by temporarily halting the development of secondary sexual characteristics, essentially widening the temporal window for gender clarification.
As far as your other, uh, “point”? Statistically, maybe, but do you know that this is the case for the individuals concerned with the topic of this post? The author of your linked study notes the most obvious shortcoming of his research: that children raised in non-traditional families may be subject to influences not examined – things like discrimination, bullying, etc. due to their non-traditional upbringing. Consider: children brought up in homes with guns are more likely to die in a shooting. Are we therefore to assume that any house with a gun means that the kids are not loved and will end up dead? Or, perhaps, that all it means is that there’s a statistical correlation, and that further study and safeguards need to be put into practice to achieve more favorable outcomes – rather than just banning all guns?
You folks can argue all you want. I’m thankful Mr. Powers brought the this issue to our attention. I had absolutley no clue this was happening in South Dakota!!!
I’m also thankful Rep. Deutsch is planning to introduce legislation “protecting South Dakota children from dangerous, unscientific and life-altering medical procedures pertaining to sex and so-called gender identity.”
Before reading this post and before following the links of contributors, I could have gone either way with my vote. Now, with the proof this is actually happening TO CHILDREN in South Dakota, I’m fully on board. If people want to have this done, they should wait until they are an adult. My job as a legislator is to protect our children.
Ban circumcision? Ear tubes? Scoliosis surgery?
No Ike, just dangerous, unscientific and life-altering medical procedures.
What? All the things I just listed fall under those same criteria. They all come with risks, are life-altering, and depending on which studies you want to cherry-pick, “unscientific”. BAN BRACES! CHILD MOUTH ABUSE!
We have been thru this before every year and they all turned out to be seeking solutions to problems that do not exist with baseless fear mongering that have little to do with what is actually happening. Problem is that real people are getting hurt from this annual dog whistle politics distracting us from the real issues South Dakota faces.
Aren’t there already laws in place for that?
I don’t normally read the Nation but this is a great article and just re-enforces a negative image of South Dakota. It hurts economic development and our economy is already suffering as it is.
How Did South Dakota Become Factory for Anti-Trans Legislation?
https://www.thenation.com/article/south-dakotan-anti-transgender-legislation/
South Dakota leads the nation in many ways including campus free speech. South Dakota should also lead the nation in preventing child abuse like this.
“Child abuse”? Holy dog whistle, Batman! Is it “child abuse” to get braces for your kids’ teeth?
Ike, it’s already illegal in SD to mutilate the genitals of a young girl. This will simply add to our current law to prevent child abuse.
What about boys? We can still hack off bits of their junk, right? Why is that okay? What kind of monster are you that you support mutilation of infant boys?
For more on Ike’s arguments, see: https://en.m.wikipedia.org/wiki/Straw_man
Explain how circumcision differs from gender reassignment therapy vis-a-vis parents seeking medical treatments for their children
Hopefully, we can learn from North Carolina.
The first difference that comes to mind is that circumcision leaves male genital function completely intact as an organ of the male reproductive system. That means the ability to successfully engage in a reproductive act, Ike. Your so-called therapy deliberately obliterates the 13 year old patient’s reproductive function. Circumcision doesn’t sterilize.
So why the ban on female circumcision?
Anonymous 9:09 references male genitals. In 2015 the legislature passed HB1089 making it a Class 4 felony for any person to “knowingly circumcise, excise, mutilate, or infibulate, in whole or in part, the labia majora, labia minora, or clitoris of a female under the age of eighteen years.” The bill passed 61-6 in the House and 34-0 in the Senate. 100% of Democrats in the House and the Senate supported it. All Republican supported it except for six in the House.
Well, that’s certainly the “what”, but my question was the “why”. FGM leaves reproduction intact. WHY is that particular procedure banned, but not for male children? You KNOW the answer: religion. FGM is largely a west African tradition (and now, largely Islamic, but that has little to do with FGM), whereas MGM is a Hebrew tradition. Just more hypocrisy.
…and also, puberty retardant hormone therapy is completely ‘reversible’ and has no effect on future reproduction. Y’all added the testosterone BS on your own.
Not so Ike. Please stop spinning. We’re talking about the life and health of a 13 year old child. A second physician has now posted on this thread.
Yeah, you did add the testosterone, and a whole host of other dubious conclusions about this family and this young person.
Changing sex on a birth certificate, change of name, and cross-sex hormones are part of a controversial treatment protocol for gender dysphoria, called “gender-affirming therapy.”
While it is impossible to be born in the wrong body (“boy brain” in a girl’s body), some children believe this has occurred to them, and this causes distress. The medical term for this distress is gender dysphoria.
Before approximately 2010, these children received supportive counseling. This approach resulted in the resolution of the gender dysphoria 85% of the time by age 20. Those that continued to have gender dysphoria would sometimes choose to have their bodies altered with hormones and surgery so that they looked like the opposite sex.
Over time, troubling trends were observed in those who had undergone such treatments. They were dying at much higher rates than the general population from suicide and other medical problems thought to be due to taking hormones that were not designed for their bodies (heart disease, strokes, blood clots, and cancer).
In an attempt to improve the long term mental health of people suffering from gender dysphoria, a group of clinicians in the Netherlands, with little scientific foundation, began medically blocking the pubertal development of children with gender dysphoria. They thought they could tell which children were unlikely to have resolution of their dysphoria by adulthood. But they couldn’t and still can’t. Nobody actually can.
This shift marked the practical beginning of what’s called “gender-affirming therapy,” which is flawed in two significant ways.
First, as I stated above, 85% of children, if allowed to go through puberty uninterrupted, will have resolution of their dysphoria.
Second, “gender-affirming therapy” makes no effort to help a child or adolescent understand the underlying causes of their rejection of their male or female body. This is a key overlooked point. Gender dysphoria always has an underlying cause, but being born in the wrong body is not one of those causes. The actual causes stem from familial, or social, or developmental roots, have been described in detail and can respond to supportive counseling.
The consequences of the broad adoption of “gender-affirming therapy” are significant. If initiated early in puberty, puberty blockers and hormones result in permanent infertility. Irreversible physical changes from the hormones and surgeries occur. It is important to state the following again: this shift from supportive counseling to gender affirmation therapy has occurred despite a lack of scientific evidence that this approach helps the long term functioning of gender dysphoric children.
Also, it is not possible for children and adolescents to have an understanding of the long term consequences of these decisions, as human brain development is not complete until the early twenties.
For the above reasons, gender-affirming therapy (including changing birth certificates, names, and administering hormones and surgeries) should not be applied to children and adolescents.
When medical professionals fail to educate patients and patients’ families about the realities of such treatments, it is not surprising that lawmakers will feel compelled to stop them.
For more reading on this topic, please see the following links:
https://thevelvetchronicle.com/no-child-born-in-the-wrong-body/
https://www.scribd.com/document/421298610/Gender-Dysphoria-Resource-for-Providers-3rd-Edition
One hyperlink at a time please, otherwise it gets caught in spam filter.
Excellent write-up! I appreciate your points, however you fail to fully address the mental health side – that these hormonal treatments are not performed in a vacuum. Therapy is a major component of gender transition. Puberty blockers administered at the correct time add significant time to allow for successful therapy, and allow the child to “be sure” of their dysphoria. I agree with your assertion that these treatments can cause significant issues down the road, but the extra couple of years for evaluation and treatment should not be overlooked.
I am interested in your point that it’s “impossible to be born in the wrong body”. Studies of identical twins show that if one twin has gender dysphoria, that the other is 40% likely to be as well, whereas with fraternal twins, the rate is only 4%. This would indicate to me that there is a genetic component to the malady. Can you discuss your opinions on that particular area of research?
(Ike, sorry, not sure why this was moderated. I think I’ve got it fixed though.)
Briefly, the few studies on puberty blockers show that rather than buying time, most, if not all children go on to the next stages of therapy. In addition, puberty blockers have not been studied in the context of halting normal puberty. There are legitimate concerns about the effects of halting normal physical( example: bone density), emotional, and intellectual development of a child during the vital years of pubertal development. Puberty blockers are described as fully reversible, but they have not been proven to be so in this context.
To your second question, I would refer you to the first hyperlink in my original post. There I discuss the twin studies. To summarize, there is a wide distribution of natural behavior within each sex. At the outer distribution of that natural behavioral, some children could incorrectly come to believe that they are the opposite sex, because their behavior is more similar to the opposite sex than to their own. But behavior does not determine one’s sex. Twins share DNA, and similar environments. Their behavioral and personality profiles are more likely to be similar. Therefore, if their natural behavior and social environment were to cause gender confusion in one twin, it would be more likely to cause confusion in the other, explaining the higher correlation of a transgender identity.
Appreciate your well-reasoned response! A couple of things, though:
“…rather than buying time, most, if not all children go on to the next stages of therapy.” do you have a source to justify that statement? I’m not sure that sounds like the whole story – I could see “a significant number” or “many”, but “all” really doesn’t leave any room for scientific method or inquiry, Doc.
I agree with much of your 2nd paragraph – there appears to be a dearth of info regarding environment and social factors in gender dysphoria. However, there are other studies which do find certain genetic markers which indicate a higher prevalence. https://www.ncbi.nlm.nih.gov/pubmed/30247609 – again, it sounds as if you’ve got your mind made up? Not trying to cause any problems, it’s just that I don’t wish to jump to any conclusions, and I certainly can’t draw any from what little we’re given from the original post/legal proceedings.
…and for the record, if you are who you say you are (I have no reason to doubt it), we all here should thank you for your expert analysis. I have learned quite a bit today! Thank you!
🙂
My mind is made up that unproven medical protocols that result in sterilization should not be applied to minors.
In the spirit of continued open and honest conversation, I have a few questions for you. I think your answers would help those reading your responses understand your perspective on this issue. And since your profile is anonymous, it should be no trouble for you to answer.
1. What is your definition of a man and a woman?
2. Can men get pregnant and deliver children?
3. Is sex assigned, or observed at birth?
4. Should biological men be allowed to participate in women’s sports? (not asking about intersex conditions)
I do think there a multitude of treatments that minors undergo that do result in sterilization which have nothing to do with gender issues – so there’s a question as to your reasoning perhaps. I sort of see where you’re coming from (your bullet list of questions makes it rather obvious), so I can only conclude that your faith is important to you and your approach to medicine. I don’t have a problem with that per se, but I did want to be clear. With that said, you’re 1200 miles away from any of this. That doesn’t affect your opinion of course, but it does call into question your motive.
As far as your questions:
1. This is a flawed question – you’re looking for physical traits? If we say “All men are created equal”, do we mean only men and not women? These definitions – legal, colloquial, societal, etc. all have limitations. I’ll just say that a “man” is anyone who believes they’re a “man” and a woman is anyone who believes they are a “woman”. Gender is a sliding scale, not a yes/no.
2. As in my first response, I’ll just say that mankind has been reproducing since forever.
3. Sex is determined in utero. There are plenty of cases where the binary sexes are not clearly defined there, however. Again, sort of a spectrum, not black and white.
4. I don’t like your definitions, but if you’re asking if a person with traditionally “male” characteristics like denser muscle mass, higher testosterone levels, etc. should compete against the ‘opposite’, I would say that’s a case-by-case basis. Blanket rules suck, and I think generally we do a pretty good job of sorting out unfair competition. There are outlier cases, and this does need discussion – but then again, the Saints should have made the Super Bowl last year, so what you gonna do?
Ike, thank you for your candid answers. However, I must point out that your positions are not based on our current understanding of biology. A few additional comments: my opposition to gender-affirming therapy has nothing to do with faith nor religion, and this issue is a national one.
No child is born in the wrong body. On average, 85% of children with gender dysphoria have resolution if allowed to go through puberty. Puberty blockers, hormones, and surgery are neither needed nor proven to improve the long term mental health of children with gender dysphoria. Instead of helping a child understand the root cause of their dysphoria, hormones, and surgery reinforce the incorrect idea that something is wrong with the child.
Also, the hormones are powerful. Testosterone, for example, permanently changes the appearance and voice of an adolescent girl, and if given early in puberty, results in life-long infertility. Children are not capable of understanding the implications of such interventions at a young age. The use of these interventions in children has rightly been called experimental and should be opposed.
I guess I have a problem with the conflation of biology and psychology. Sex and gender are separate in some cases, and you’re leaving 15% of these cases to the winds. These are the marginalized people at the heart if the legal issues this post is tackling. The rules don’t have to be one-size-fits-all. Our school administrators in SD have been doing a good job so far. I see no need for the legislature to get involved.
Biology is the essenece of life. Biology dictates if the person is male or female. School administrators have nothing to do with this case becasue it has nothing to do with education.
Minors under age 18 shouldn’t be making life altering decisions like this. Our society should protect children, especially if they are marginalized and more vulnerable than usual, from unproven and irreversible medical interventions.
Nice ad hominem attack, Donna. Instead of genuine discussion of the topic at hand, you avoid it by instead attacking the character of the person making the argument. You can do better than that Donna.
Donna, while you are correct about where I practice, everything else you’ve stated is false.
Regardless, I’d be happy to engage you on the issue at hand.
First though, as I asked “Ike” above, I think it’s important to know where you are coming from on this issue. Both for myself, but also for those who may read these posts. So, several easily answered questions for you, which I’ve answered in one form or another in the links to my writings in previous posts:
1. What is your definition of a man? A woman?
2. Can men get pregnant and give birth?
3. Is sex assigned at birth by a doctor, or observed and recorded?
4. Should biological men be allowed to compete in women’s sporting events?
5. Can a boy be born in a girl’s body?
SPLC co-founder, Morris Dees assaulted his wife and tried to molest his step-daughter. Dees was fired.
SPLC president, Richard Cohen, resigned amid accusations of racism and sexism. Two dozen employees reportedly signed a letter to management and the center’s board of directors detailing “allegations of mistreatment, sexual harassment, gender discrimination, and racism.”
Rhonda Brownstein, SPLC’s legal director, resigned as well.
Twitter dropped SPLC as one of their ‘Safety Partner’.
Senator Tom Cotton to IRS: “I am writing to urge you to investigate whether the Southern Poverty Law Center (SPLC) should retain its classification as a 501(c)(3) nonprofit organization. Recent news reports have confirmed the long-established fact that the SPLC regularly engages in defamation of its political opponents. In fact, the SPLC’s defining characteristic is to fundraise off of defamation. According to the group’s most recent financial statement, it holds $121 million offshore in non-U.S. equity funds. The SPLC uses these assets to pay its executives lavish salaries far higher than the comparable household average.”
This is the organization “Donna” finds to be credible?
“Donna” was posting from a proxy server, which isn’t allowed. And I suspect it was because they’ve been long banned.