From Twitter, outgoing State Senator Erin Tobin who had previously been an advocate for unsuccessful efforts to bring exceptions to South Dakota’s total abortion ban in cases involving the health of the mother is pointing out today that Winner South Dakota will no longer offer labor and delivery services at Winner Regional Health:
Should this become a trend, the lack of OB/GYN care in rural settings should draw our lawmakers’ attention, as our state’s infant mortality rates are increasing and seems to be skyrocketing among Native Americans, having more than doubled in that population group since mortality hit a low in 2017:
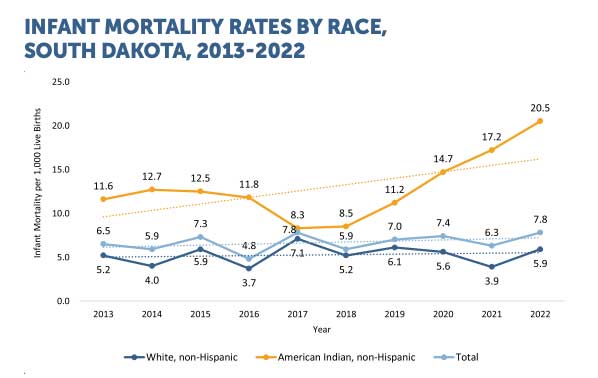
https://doh.sd.gov/media/mr4otnoy/infantmortality_1pager_2024.pdf
Add a lack of medical services to a lack of child care, lack of jobs, declining schools, and the other things that negatively impact rural South Dakota communities.
We are among the top five states people are leaving. The tax burden is on homeowners in town, and they use the tax to enforce the country people’s delusions on everyone. I’m not surprised.
Well we are talking about physician recruitment here. A physician’s biggest burden is income tax and here in SD we don’t have one. This would allow a physician to keep around 7% of their income in their pocket here.
However, maybe physician recruitment has a little to do with 1. The strictest regulations on pregnancy care in the whole nation 2. A whacky legislature that will not even compromise with ACOG to talk about their concerns about women carrying babies and how to address those without being thrown in prison 3. A part of the Republican Party that is so out of touch that they would like to get rid of basic immunization requirements catapulting our state back into a measles epidemic PLUS charge a medical provider with a misdemeanor if they do recommend vaccines (Qualm 2019 – who is now running for the GOP chair).
If I was a resident doctor, especially an OBGYN, I may decide to take that 7% hit on my income tax and go practice where I won’t be thrown in prison.
Well, our new prison will be pretty nice, and maybe we will improve our work release option. If we offer (or force) room and board for physicians, we can pay them prisoner wages $.50/hr, but charge market rate to the patient. The profit can go to the GOED fund which can’t be tracked (need to kill SB10 first) and that can go back to the donors as a return on their investment. This doesn’t sound like too bad of an option, we would need the Unruhs’ and Hansen to write the specific rules for these prison doctors to practice biblical medicine, but we won’t have a shortage anymore once we do this.
Well, that was a stupid comment.
It will be even more stupid once implemented, and the SD MAGA’s will applaud it.
See prior comment.
Whelp, we’re primed this session to double down on gutting rural schools and continue doing nothing for child care, elder care, and stemming the outflow of all the obgyns.
#winning
Noem’s policies & plans were written on jet criss crossing the country. Governor of the flyover state
Lots of finger pointing above, but this really isn’t a brand new occurrence. Rural SD has struggled to bring doctors of all kinds back home. Also – doctors, lawyers and many other professionals would prefer to live in Sioux Falls and Rapid City. Again – nothing new. Been happening for lots of years. To blame it on tax policy or pro-life stances is a bad argument. A lot of young people simply don’t want to live in our small towns and not just Winner.
When the total population of a county is less than 6000 people and essentially ALL the pregnant females are on Medicaid, it is impossible to sustain an OB-GYN practice. Not many doctors want to work for free. Medicaid expansion has its downside. Who knew?
I was working at the Flandreau Hospital in the early 1990s and they were still delivering babies there. I thought it was NUTS. The family practice physicians couldn’t do emergency C-Sections, and surgical staff not even kept on call. .
The Director of Nursing was caught between the Joint Commission’s requirement that emergency c-sections should take no more than 30 minutes, & the Board of Directors’ belief that the public’s perception of the place as a hospital would be diminished if they didn’t deliver babies there.
The nearest surgeon was 30 miles away in Brookings and could not possibly make the trip, scrub in and pull out a baby in less than 30 minutes. Personally I thought 30 minutes was way too long to rescue a baby from a placental abruption or cord detachment, but in any case, the idea that the board members were more concerned about public relations than babies was really disturbing.
The babies won and deliveries at that hospital ceased. Moody County moms go to Brookings or Sioux Falls.
Winner is a one-hour drive from Chamberlain, where Dr Cynthia Davis has an ob-gyn practice.
Deal with it.
Anne – All of the above issues contribute to one big cluster of a situation. Winner is the last standing provider who provides OB care to Mission, Rosebud, St. Francis and further west- which are even further away from Chamberlain and there isn’t ability for some of these people to travel.
Yes, many of these are poor people. Does that mean they are less deserving of prenatal care/OB care and should have to deal with it? Does that mean that those babies deserve to die of syphilis or spina bifida? I don’t think saying “deal with it” is a responsible solution. We are living in the 21st century and we can do better for maternal child death and other health measures/outcomes.
All children deserve to be born without preventable diseases and have the best start to their life, even if their parents are underserved and poor. To be prolife you also have to care about preventing death. Otherwise – you are contradictory.
Constructive discussion and coming to the table with multiple solutions and an open mind will be necessary to find solutions.
Living many miles from medical care is a CHOICE. When I lived in McLaughlin I had to drive 90 miles to Bismarck to see an obstetrician and give birth at St Alexis Hospital.
I was not confined by county or state lines. Living in rural South Dakota and going to North Dakota to give birth was my choice.
If people CHOOSE to live in the middle of nowhere, they will have to deal with the consequences of that decision.
If they don’t want to live many miles from the care they want, they can move. I do not understand why this needs to be explained to anybody.
With all due respect….unless you are poor and confined to a reservation.
I believe we can make positive steps and keep care in our small towns whether it is family practice or OB when it makes sense. Those positive steps are legislative efforts, recruiting efforts by health care systems, and efforts by our universities to educate and retain. I think consolidation of administrative duties may be helpful in rural areas as well.
Nobody is confined to a reservation, the reservations are not internment camps. They can leave any time they want; the residents live there entirely by choice.
When I arrived on Standing Rock, and was given tge grand tour of Ft Yates, I asked the hospital administrator “why do people live here? ”
He could only say “it’s their home.” Okay, so why not find a different home? No explanation.
Anne treating moving hours away from all you’ve ever known with probably zero money as though it’s as easy as trimming your fingernails.
This is grand, two autocrats arguing about choice, LOL.
Anne – medicaid expansion did not expand to include pregnant women. Medicaid always include those carrying babies because of the child’s needs.
The hospital statement references problems with reimbursement. How much of that is unpaid bilks from the IHS?
One thing I don’t know the details of: “Effective July 1, 2023, the limited coverage pregnancy group was transitioned from a limited benefits group to a full coverage group.” Does that mean they get more or less money? And how long does the transition take?
IHS patients almost always qualify for Medicaid. State Medicaid reimbursements follow federal guidelines which set an upper and lower limit of reimbursement. Services are reimbursed for deliveries but reimbursed better if there is both prenatal care and then delivery.
But maybe these people should just move to Sioux Falls. The farmers and ranchers who live in rural SD should just sell the farm and move to Sioux Falls too following your logic.
yes maybe they should move to the cities.
Life on the reservations is bad. Everybody knows that.
We all hear about how terrible it is. For one thing, winter is always a surprise. Nobody ever knows that summer is going to end, so they don’t get their propane tanks filled. The social justice warriors, who could go door to door in August asking if the propane tanks are full or the firewood is stacked, and could offer assistance to those who need it, don’t appear until January or February, and then only to complain that nobody told them that winter was going to happen again.
Then we have to hear about the boondoggle that is the IHS. The Ft Laramie Treaty promised one doctor in a $3000 house by the river where timber is plentiful. No hospitals, clinics, pharmacists, nurses, lab techs; just one doctor, a general practitioner, living in a $3000 house (van?) down by the river. Mission creep on steroids. Now they are complaining because they don’t have specialists??
If you don’t like your living conditions, MOVE.
Being a resident of Chamberlain, I continue to hear that the IHS doesn’t/won’t pay and if they do they are extremely late to pay. Even our own ambulance service has to write off there transportation/emergency services that involves the IHS. Guess who it falls back on – the local taxpayers. We have a real crisis brewing with our reservations and no one wants to step up and fix it. Even the Native American populations are oblivious to it.
i have never been so happy to stay out of an argument.
Good choice…you would be wrong anyway…as usual.
Just today I also read that Volga pleads for more people to join the volunteer fire department. And the Wessington Springs legion hall is being foreclosed on for not paying their loan because they don’t have as many members. The decline of rural SD has been happening for decades and will continue to happen. This is not about physician recruitment. It’s about demographics, mobility, the need and desire to have larger farm operations in order to be successful, cultural shifts, and changes in where people want to live. Physician services is a symptom of broader changes happening.
Throw in the ‘no on everything growth’ stance which leads to less payers and more local effort. Number one complaint is property taxes yet many rural counties oppose any new growth or development. So if you don’t have growth and the people are not willing to pay more taxes you will have school consolidation, then county consolidation, then small towns and townships dissolving. This Republican Party and this NO mentality will kill what everyone claims to love the most, small town South Dakota.